Who chooses to have breast reduction?
Most women who desire a breast reduction simply feel that their breasts are disproportionately large and heavy. For many women this makes it difficult to find clothes which fit properly, particularly dresses. Some women with large breasts develop “shoulder grooving” from the bra straps, and rashes under the breasts in hot weather. Others complain of back and neck pain and feel that the heaviness of their breasts is causing postural problems.
Some women develop very large breasts during puberty; others find that their breast size increases after having children or following the menopause.
A breast reduction will not prevent breast pain, as there is still plenty of breast tissue left after the operation, but some patients find that the heaviness associated with their pain is better after surgery.
A breast reduction will not prevent you getting breast cancer, though there is some evidence that reducing the amount of breast tissue can reduce the risk of cancer slightly. It is important to remember that mammograms will be less accurate after a reduction because the scar tissue inside the breast can mask a very small cancer, and you should tell your mammographers that you have had reduction surgery.
For more information from the Association of Breast Surgery, BAPRAS and BAAPS websites on breast reduction.
Preoperative Assessment
During the initial consultation I will discuss with you your reasons for wanting a reduction, and how much smaller you would ideally like to be. It is not possible to guarantee a particular bra size afterwards, due to the different ways bra size is calculated. The procedure is designed to make your breasts proportionate with your trunk, so the final size will depend to some extent on your overall size.
I will discuss with you the risks and complications of breast reduction surgery and what to expect afterwards. You will be shown photographs of the procedure and the results. There are several different methods of performing a breast reduction and I will discuss which of these are appropriate for you.
If you are 40years or older a preoperative mammogram will be ordered.
Types of Breast Reduction
Although it is possible to reduce breast size in some women by liposuction alone, I do not generally advise this, as it dos not incorporate any form of uplift, and so does not give very good overall results.
In small-breasted women who need a small reduction in order to improve symmetry, then it is sometimes possible to use the Benelli technique, which leaves only a scar around the areola, the pigmented skin around the nipple. This type of reduction does not work for moderate or large breasts.
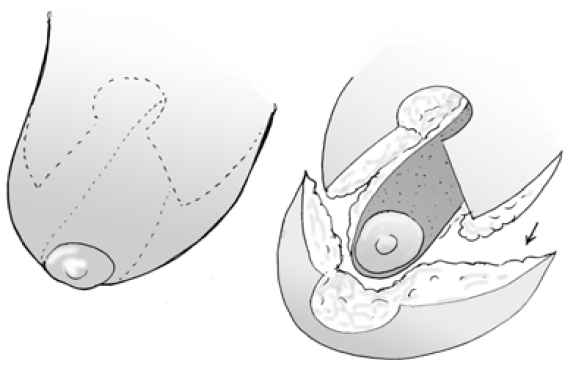
The commonest type of breast reduction performed in the UK is the inverted T, or Wise pattern, technique, which leaves a scar around the areola, down to the crease under the breast and along the crease from end to end. Like the Benelli, this technique is dependent on the breast skin to hold the shape of the breast. Over time, the skin tends to stretch and the breast “bottoms out”, leaving most of the breast tissue sitting below the level of the nipple, rather than behind it. In extreme cases, this can lead to difficulty wearing a bra, as the high-riding nipple is pushed out of the top of the bra cup.


Post Operative
You can expect to stay in hospital for 1 night after the operation. You may require drains overnight which are typically removed before you go home. You are likely to experience some discomfort, but this can usually be controlled by normal painkillers. You will be sent home with antibiotics to take to prevent infections. It is recommended that you wear a sports bra day and night for 2 weeks after the operation and then during the day for a further 2 weeks
You are likely to have paper tape dressings over the wounds which should be left in place until you are seen in the clinic at around 1-2 weeks. These are showerproof and should simply be patted dry after bathing. They may start to look a little frayed by the time you come back to the clinic, but it is best to leave them in place for the first few weeks, rather than changing them.
You will be seen in the clinic 2-3 weeks after surgery, to check that your wounds have healed well and that you have developed no other problems. You will be advised to continue wearing the dressing tape for as much time as possible over the next 3 months, as this helps to keep your scars from widening. You can change the tapes yourself every week or so during this time. You will be seen again at 3 months and 1 year postoperatively.
Complications / Side Effects
Breast reduction surgery involves a general anaesthetic and takes 3 hours. The usual risks of a long operation are therefore present. These include both chest infection and deep vein thrombosis (clots in the legs that may spread to the lungs – pulmonary emboli, which whilst very rare, can prove fatal). Steps are taken to reduce the risks and these include the use of compression stocking and early mobilisation.
Sometimes bleeding occurs in the hours immediately after the operation. This usually makes one breast more swollen and uncomfortable than the other. Sometimes it is necessary to return to theatre to remove the haematoma (blood clot) and stop any further bleeding.
Nipple sensation
The nipples and breast will be numb after the operation. As sensation returns you may experience sharp shooting pains. Sometimes not all the sensation returns, particularly in the nipple, which may lose all or some of its sensitivity, including erotic sensation. Occasionally patients describe increased nipple sensitivity after breast reduction. These changes may not be symmetrical.
Nipple Necrosis
There is a very small possibility that the nipple may lose its blood supply and become necrotic (the skin may become black and heal by scarring with loss of pigmentation) or you may even lose the nipple in extreme cases. This is extremely rare. Nipple reconstruction can be performed at a later date, and loss of pigmentation can be corrected by tattooing.
Infection is another possibility despite the routine administration of antibiotics during the procedure. If you do get an infection, the scars can become a little thicker and the eventual scar you are left with may not be like the one you are shown pre-operatively. Even without infection some women develop thick unsightly scars due to a condition called keloid. Special silicone dressings may be required to treat these scars. The scars may also become quite broad.
Fat necrosis occurs when a part of the breast tissue that is left behind does not have a good enough blood supply. It usually takes the form of small lumps just beneath the scars which are noticed about 2-3 months after the operation. Rarely, a large area of the breast can go generally firm. The condition is benign and does not carry any risk of cancer, and often settles with time. Lumps that do not resolve can often be removed.
Returning Home
Once discharged home, you can bath or shower as normal. The stitches in your wound will dissolve. The dressings are left until the first clinic appointment. An appointment will be made for you to come back to clinic about 2 weeks after discharge. You can expect bruising and swelling in the breasts and will be hard and swollen for some weeks.
